
Korea’s rehabilitation gap: why critically ill patients struggle without institutional support < Hospital < Article

The reality of healthcare in Korea becomes more apparent when it is compared with developed countries. Nowhere else is this more salient than the rehabilitation therapy for severely ill patients.
In Korea, rehabilitation for critically ill patients is maintained by the efforts of medical professionals without reasonable medical fees or institutional support. In contrast, in developed countries, the government supports it with fees and other systems, and medical workers strive to find better treatment within such a system where rehabilitation for critically ill patients is taken for granted.
In developed countries, including the U.S., Canada, and Europe, rehabilitation treatment in intensive care units is taken for granted. Early rehabilitation of critically ill patients has become the standard of care, as various studies have shown.
According to the international journal Critical Care, a 2019 survey of 591 U.S. hospitals found that 66.5 percent of ICU patients received physiotherapy.
Among them, 41.0 percent received occupational therapy, and 32.2 percent received speech therapy. Most ICUs in the United States have adopted early rehabilitation as the standard of care.
Many European countries also have extensive experience with ICU rehabilitation. Guidelines are in place. Germany and Switzerland have established intensive care coordination systems for early rehabilitation. Critical care specialists, physiotherapists, and nurses work together to provide rehabilitation for critically ill patients. The same is true in Australia and New Zealand. Most ICUs have at least one senior physiotherapist in the two Oceanic countries.
More than 50 percent of hospitals with ICUs in Japan reportedly have early rehabilitation programs. The results are clear: 56 percent of critically ill patients on ventilators recovered enough to sit on the edge of the bed within five days of admission to the ICU.
This was the conclusion of a study on early rehabilitation and early mobilization in intensive care published in the international journal Scientific Reports in 2023. Japanese researchers conducted a multicenter retrospective cohort study of patients admitted to six intensive care units between April 2019 and March 2020. Patients aged 18 years and older who had been mechanically ventilated for more than 48 hours had a 56 percent rate of early exercise achievement. Early mobilization was defined as the ability to sit on the edge of the bed within five days of ICU admission.
“Early rehabilitation in the ICU is being actively studied worldwide. In many countries, especially in the U.S., rehabilitation of critically ill patients is already standard of care,” Professor Chung Chi-ryang of the Department of Critical Care Medicine at Samsung Medical Center said. “Many studies have shown that early rehabilitation plays an important role in the critical care process.”
Professor Hyun Sung-eun of the Department of Rehabilitation Medicine at Seoul National University Hospital said, “In developed countries, rehabilitation in intensive care units is commonplace. Not providing rehabilitation for critically ill patients is perceived as an act of harm to the patient.”

In developed countries, sufficient specialists offer various rehabilitation treatments
A wide range of rehabilitation treatments is available in developed countries, and the number of specialized staff is also expanding.
“Countries with universal critical care rehabilitation have dedicated mobility teams and multidisciplinary teams, including critical care physicians, rehabilitation physicians, nurses, critical care rehabilitation coordinators, physiotherapists, occupational therapists, and speech therapists,” Professor Chung said. “They are different from Korea because they have more people, training, and equipment.”
In the U.S., Australia, and European countries, intensive care units are staffed exclusively for rehabilitation, provided in the morning and afternoon, even on public holidays, Chung explained. For each unit (eight to ten beds), there are two to three dedicated physiotherapists. He added that dedicated occupational therapists, speech therapists, and critical care rehabilitation assistants are also assigned to ensure comprehensive rehabilitation.
Professor Kim Tae-yoon of the Department of Critical Care Medicine at Ewha Womans University Seoul Hospital said, “In Japan and the U.S., the types of rehabilitation provided are more diverse than in Korea,’’
In Korea, some ICUs provide not only physical therapy but also occupational therapy and speech therapy. However, in Japan and the U.S., multidisciplinary rehabilitation, such as physical, occupational, and speech therapy, is systematically provided, Professor Kim explained. However, since the U.S. is based on private insurance, the composition and scope of rehabilitation therapy varies depending on each hospital’s system and the patient’s insurance criteria, Kim noted.
Developed countries are also expanding the scope of critical care rehabilitation from adults to children. The U.S. Society of Critical Care Medicine (SCCM) published the PANDEM Guidelines for Infants and Children in 2022, recommending “early mobilization” for pediatric patients to actively manage pain, anxiety, and delirium and keep them awake and moving as much as possible. PANDEM stands for Pain, Agitation, Neuromuscular Blockade, Delirium, and Early Mobilization.
“SCCM recommends setting appropriate mobility training goals for individual patients daily, considering the changing conditions of patients in the ICU, and inducing as much functional movement as possible, reflecting their developmental age,” Professor Hyun said. “European countries are also actively implementing early rehabilitation in pediatric ICUs, and the National Health Service (NHS) guidelines strongly recommend rehabilitation for critically ill patients.”
Supported by fees and policy, early rehabilitation of critically ill patients has become commonplace
The ubiquity of early rehabilitation for critically ill patients in developed countries owes to rational healthcare systems. In developed countries, the government actively supports the efforts of medical staff with fees and policies.
Japan, which has a similar healthcare system to Korea, also encourages rehabilitation for critically ill patients through fees and systems.
According to the Korean Society of ICU Rehabilitation, Japanese hospitals can bill insurance companies directly for $34.6 (about 50,000 won) per day for the first 14 days after admission to the ICU. From the 15th day onwards, they can bill up to six times daily, ranging from 1,750 yen (about 16,700 won) to 2,450 yen (about 23,400 won) per 20 minutes, depending on the condition. Korea does not have a fee for rehabilitation for critically ill patients. Even if it does, it must apply the simple exercise therapy fee of 6,290 won ($4.3) daily.
“To bill for the first 14 days of rehabilitation in Japanese ICUs, you must have the required personnel. The required personnel include doctors and nurses with at least five years of experience in ICU care and physiotherapists, occupational therapists, and speech therapists with at least five years of experience in acute illness rehabilitation,” Professor Kim said.
The U.S. is known to have higher prices for rehabilitation for critically ill patients than Japan. “Because the U.S. is a private insurance-based country, rehabilitation costs and billing methods vary by medical institution and insurance company,” Kim said. “In general, rehabilitation costs are billed based on insurance company policies and Diagnosis-Related Group (DRG), and are generally higher than in Japan.”
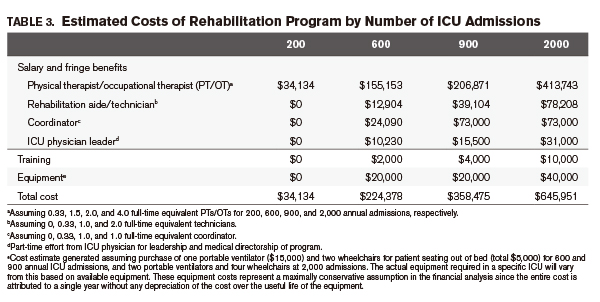
Based on the study’s results, some estimates put the cost of rehabilitation for critically ill patients in the U.S. at more than 130,000 won per person per day. According to a 2013 study published in Critical Care Medicine, if 600 patients are admitted to an ICU annually, the labor costs for rehabilitation alone total $202,377 (about 294 million won). Add to that $2,000 per year for training and $20,000 per year for equipment; the estimated cost is $224,378 per year (about 326 million won).
Professor Park Jin-young of the Department of Rehabilitation Medicine at Gangnam Severance Hospital said, “Considering that the average profit margin of non-profit hospitals in the U.S. is 3-6 percent, 335 million won should be charged even if one assumes a minimum profit of 3 percent.
Considering the average length of stay in the ICU (5.4 days at Johns Hopkins Hospital), the average cost of rehabilitation per day was 103,300 won in 2013, Professor Park noted. The U.S. consumer price index is expected to increase 1.35 times in 2024 compared to 2013, when the study was conducted. He added that the average cost of rehabilitation for critically ill patients in the U.S. is currently estimated to be 134,290 won per day.
In some countries, rehabilitation is included in treating certain conditions in intensive care units. “Some countries have implemented comprehensive systems that bundle rehabilitation for specific groups of patients admitted to ICUs,” Professor Kim said. “Several countries, including Sweden and Norway, provide bundled rehabilitation for patients admitted to ICUs with central nervous system diseases.”
Kim said that following Japan’s example, Korea should also make rehabilitation for critically ill patients a covered service.
“In the U.S., private insurance provides coverage in proportion to the amount of capital invested, but this is not possible in Korea,” Professor Kim said. “Realistically, it is necessary to review the composition of the required manpower by referring to the Japanese case, calculate the amount per session, and provide physiotherapy, occupational therapy, speech therapy, and others in a bundle or multidisciplinary approach based on this.”
Rehabilitation therapy expands to pediatric patients overseas. What about Korea?
Developed countries have gone a step further in considering and implementing ways to increase the acceptance of rehabilitation for critically ill patients. Countries such as Germany, Canada, and Australia have established guidelines for rehabilitating critically ill patients and are educating medical staff. The Japanese Society of Intensive Care Medicine did so in 2023, and the European Society of Intensive Care Medicine also published guidelines for 2024.
They also strive to raise awareness among healthcare providers. One example is the “PICU UP!” program at Johns Hopkins Hospital in the U.S., conducted in the Pediatric Intensive Care Unit (PICU). The program aims to provide rehabilitation to every child every day. It was started 10 years ago by physiotherapists, respiratory rehabilitation therapists, occupational therapists, speech therapists, nurses, and child development specialists from pediatrics, inpatient medicine, rehabilitation medicine, anesthesiology, and pain medicine.

“The success of the ‘PICU UP!’ program was because they could improve the awareness of ICU staff,” Professor Hyun said. “They focused on sharing the perception that ‘no child is too sick to do early exercise,’ and then communicated with patients and their caregivers to explain why it is important to move even during ventilator treatment, the need to stand up, and to gain the empathy of both the medical staff and caregivers.”
Professor Hyun noted that Dr. Sapna R. Kudchadkar, the team leader of the PICU UP! program, has been advocating the value of pediatric critical care rehabilitation and sharing her experiences and trials and tribulations with the world. As a result, more than 200 children’s hospitals worldwide have activated pediatric critical care rehabilitation programs, Hyun added.
“I hope that the internationally recognized pediatric critical care rehabilitation program can be introduced in Korea as soon as possible,” Hyun said. “For this, it is necessary to organize a dedicated critical care rehabilitation staff systematically.”
However, hospital executives are faced with the burden of providing such treatment, which requires a lot of resources, including manpower and equipment.
Professor Chung said, “In the U.S., studies have shown that rehabilitating critically ill patients is economically effective by reducing the length of stay in the ICU.”
Chung noted that educating doctors, nurses, and therapists on screening criteria and protocols for critically ill patients in need of rehabilitation and the prevention of “Post-Intensive Care Syndrome (PICS)” will help reduce resistance to initiating treatment. He also emphasized the need to reassign tasks so that they do not feel overburdened by the introduction of new treatments.
Professor Hyun said, “It is difficult to allocate dedicated staff within hospitals to treatments that are not paid for. In this reality, it is nearly impossible to provide a multidisciplinary approach, team meetings, and early exercise training with three or four people working together, every day, to every patient, simply because an individual decides that critical care rehabilitation is needed.”
In contrast, ICUs in developed countries adjust lighting and reduce machine noise to help pediatric patients sleep. They also use music and media to familiarize pediatric patients with the ICU.
Professor Hyun said, “In foreign hospitals, mobility training using strollers, bicycles, and kickboards is actively carried out according to the growth stage and body size, but in domestic ICUs, it is difficult to install even a small respiratory rehabilitation device due to lack of space,” reiterating the need for dedicated staff and sufficient space.
All this shows how hospitals in developed countries are constantly looking for ways to help more critically ill patients receive early rehabilitation. However, Korean doctors are more envious of the medical environment in which they can rehabilitate critically ill patients.
link





