
Fact check: Alberta’s new two-tier system is not “European” health care

The Alberta government is engaged in significant reforms that strike at the foundation of public health care in Canada. Multiple legislative and policy changes encourage greater for-profit surgical outsourcing, opening the door to for-profit hospital ownership, and dismantling the provincial health authority and fragmenting health care delivery. But it is Bill 11 that stands out above all.
Bill 11—the end of Canadian medicare?
Bill 11 fundamentally restructures both the financing and delivery of health care in the province. It is the most significant challenge to Canadian single-payer health care since the creation of public medicare.
Bill 11 legislates significant changes to health care financing (who pays for health care) by creating a private-pay market where doctors and facilities can charge patients for physician and hospital services covered under the Canada Health Act. The Alberta government claims that Bill 11 brings the provincial health system closer to other provinces and European models that allow “dual physician practice” whereby physicians can bill the public insurance plan and charge patients simultaneously for the same service. Dual physician practice is the means to achieve two-tier health care where the wealthiest can pay to jump the queue.
Among the multiple rationales for bringing in two-tier health care, the Alberta government argues that dual physician practice brings Alberta’s health system closer to those in much of western Europe and Australia. The government’s press release states that:
Dual practice exists in New Brunswick and Quebec and is widely used in countries with top-performing health systems, including Denmark, the Netherlands, United Kingdom, France, Germany, Spain, and Australia.
These are big claims that deserve scrutiny. Let’s take a look at these claims in detail.
No other province allows dual practice based on Alberta’s new model
The Alberta dual practice model does not exist in New Brunswick or Quebec. Neither New Brunswick nor Quebec have “flexibly participating physicians” who are allowed to concurrently bill the public insurance plan and work in the private-pay market. Most concerning, Alberta is the first province to allow dual practice and explicitly encourage the private health insurance market for medically necessary care.
The Alberta government decontextualizes international health systems
Every country has distinct health system characteristics, ranging from how health care is financed (who pays) and how it is delivered (who provides it). These arrangements can even vary at the sub-national level, similar to differences between provincial health systems in Canada.
There are two main forms of health system financing, which refers to who pays for health services.
For the most part, the Alberta government suggests that recent changes bring the provincial health system closer to countries with a social health insurance model (also called the Bismark model), where the health system is primarily financed through income-based contributions from employees and employers, typically through highly regulated non-profit insurers. Germany and the Netherlands are examples of social health insurance models.
The other model is the tax-financed system (called the Beveridge model) with single-payer public health insurance like Canada and Australia or a national health service like England’s National Health Service (NHS England) and the UK nations of Scotland, Northern Ireland, and Wales. The NHS is financed through general tax revenue, similar to Canadian provincial health systems. However, in each of the devolved UK nations, the NHS provides more expansive coverage, including dental, eye care, and drugs.
Within these two health system financing models, there are contextual differences between health systems in western Europe and Australia that the Alberta government is using for comparison (referred to as the “comparator countries”). Now that we’ve covered some of the basics concepts, let’s examine why Alberta’s dual practice legislation does not bring “European-style” health care to Canada:
Where private health insurance exists, it is not generally used for queue jumping
In most cases, the international health systems used for comparison by the Alberta government—Australia, Denmark, France, Germany, the Netherlands, Spain, and England (United Kingdom)—have some form of private health insurance (many are non-profit and highly regulated insurers).
However, private health insurance (PHI) is complementary or used as an alternative to the public scheme. Another type, supplementary (also called duplicative) PHI, refers to private insurance that duplicates what is offered by the public scheme. In Germany, for example, duplicative PHI serves only as an alternative to the public social health insurance (SHI) scheme intended for high-income residents.1 Once opted into PHI, it is very difficult to return to the public scheme, and you must continue paying for PHI. Put simply, PHI does not function as “queue-jumping insurance” like the Alberta model. None of the comparator health systems, with the exception of Australia, have PHI for the primary purpose of queue jumping (see Appendix Table, column D).
Another type of PHI is called complementary PHI, which refers to private insurance for services that are not covered by the public scheme. It does not serve as a parallel tier to jump the queue. In France, for example, complementary PHI is used to reimburse a portion of the costs of services that are included in the public SHI scheme. In this sense, complementary PHI is not used for faster access or better quality services than what is offered under the public SHI scheme.2
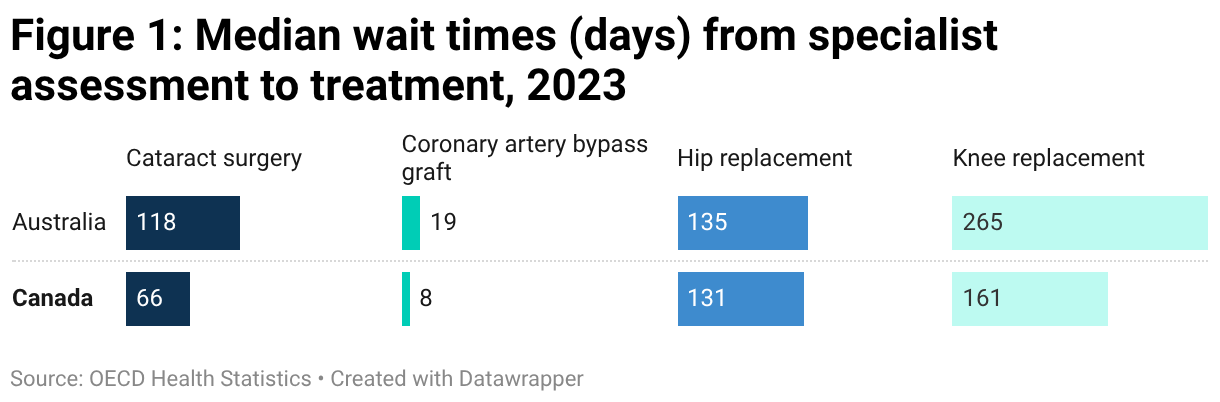
Australia—the closest to the Alberta model—provides billions in public subsidy to the private insurance industry and has longer waits than Canada
Australia has public medicare funded by the federal and state governments. About 46 per cent have PHI for hospital care, for which the federal government provides tax rebates towards coverage. High-income individuals risk penalties if they do not purchase PHI. In 2025, the Australian federal government provided $7.6 billion in tax subsidies to Australians purchasing PHI. The Australian experience with dual physician practice and duplicative PHI is a cautionary tale for Canada, considering that public wait times are generally longer in Australia than Canada for four priority procedures. Stephen Duckett, economist and former Alberta Health Services CEO, sums up Australia’s two-tier system in this way:
“In contrast to the claims by proponents, increased private provision does not lead to improved access to public care to any significant extent, nor does it reduce waiting times. It does, however, allow higher incomes for doctors and provides business opportunities for investors in private hospitals.”3
Dual physician practice is limited and highly regulated due to employment contracts
While hospital-based physicians and surgeons (called hospitalists) are allowed to engage in dual practice in some European health systems, these arrangements are often complex and highly regulated, largely due to their status as salaried employees (see Appendix Table, columns B and C). Unlike Alberta and Australia, hospitalists in the comparator countries are primarily salaried employees and have contractual obligations and limitations regarding private-pay work. Therefore, the Alberta government’s comparisons about dual practice in other countries are misleading, considering the salaried employment status of most hospitalists in the comparator countries.
Specifically, salaried employment constrains the ability of physicians to work outside of their contractual hours in the public system. It is also common in these countries for hospitalists’ contracts to limit the amount of time they spend working in the private-pay market in order to ensure that they are available in the public system. Based on Bill 11, as passed in December 2025, Alberta has none of these safeguards. Physicians and surgeons are overwhelmingly self-employed independent contractors who bill the province on a “fee-for-service” basis and have autonomy in how much they will work and where they work. Canadian doctors have among the greatest professional autonomy within the OECD.
Lower physician compensation allows for more doctors per capita
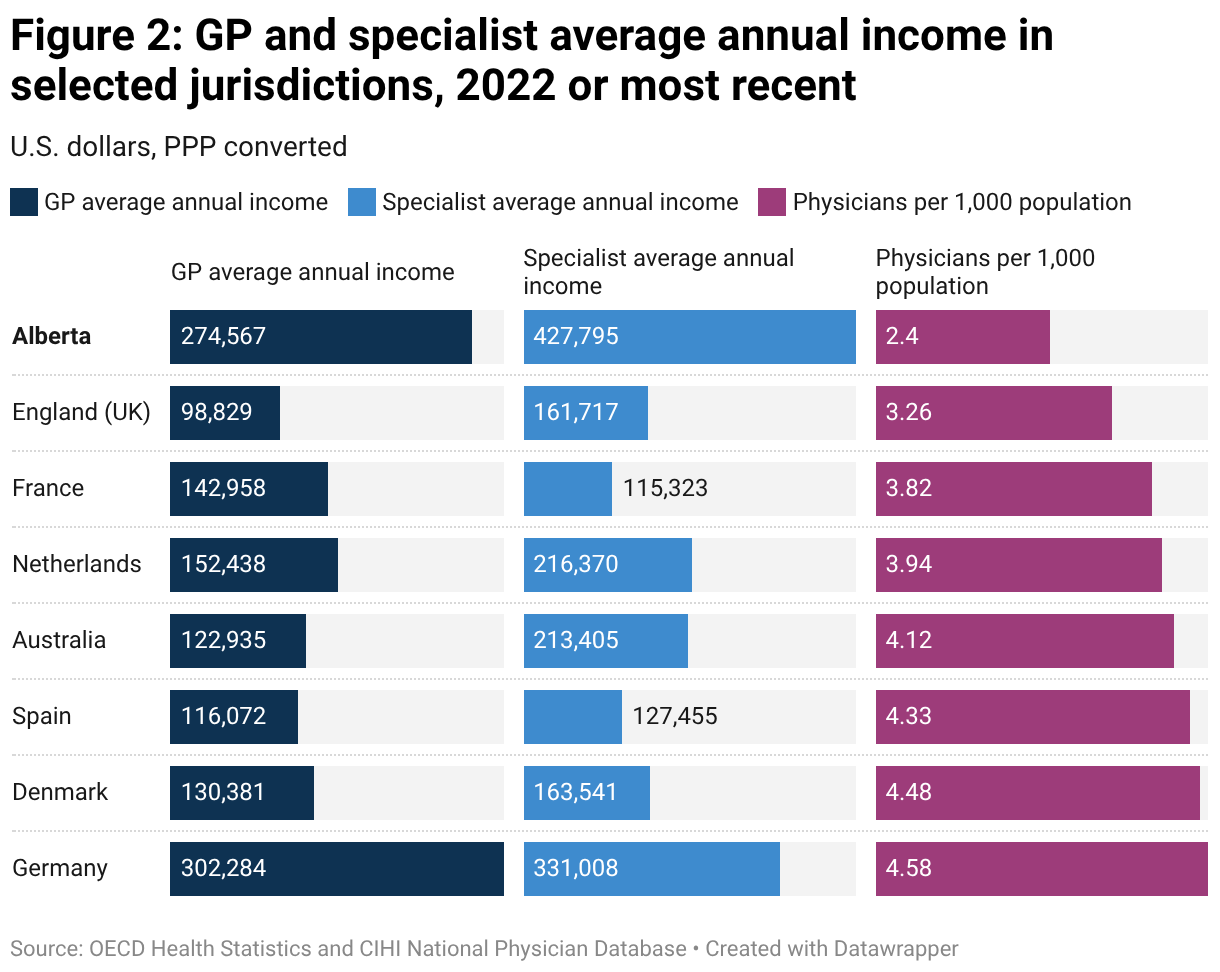
In all comparator countries, general practitioners (GPs) and specialist physicians and surgeons are paid less than in Alberta (with the exception of GPs in Germany), which means that the public system can ensure greater access to medical services (with lower pay, the system can employ more physicians per capita). As well, international health systems with more physicians per capita are in a better position to be able to allow limited dual practice because there are more physicians and surgeons to go around. With 2.4 physicians per 1,000 people, Alberta has almost half the number of physicians of some comparator countries, on a per capita basis.
In Alberta, specialists are paid an average of USD$427,795—significantly higher than next-highest, in Germany, at USD$331,008. Canadian provinces, including Alberta, offer physicians very generous compensation. Physician compensation is one of the most significant cost drivers of health systems in Canada. As a result, provincial health systems have fewer resources to pay for additional physicians and other health care professionals. These countries generally have much lower medical training costs due to much greater public investment in medical training and the health care workforce. Lower physician compensation means more physicians per capita. This is a necessary tradeoff in order to maintain a publicly financed health system and equitable access for all.
Public wait times remain a policy challenge in countries with dual practice
Public wait times remain a policy challenge—to varying degrees—for most comparator countries, even with highly regulated dual physician practice. In Australia, England (UK), Denmark, Spain, and the Netherlands, public wait times remain moderate or high policy priorities. These are countries that allow some form of regulated dual physician practice. In Australia, the closest comparison to Alberta, wait times for priority procedures remain much longer (Figure 1), and the country subsidizes the private insurance industry to a significant extent. Encouraging dual practice and two-tier health care does not magically reduce public wait times. On the contrary, the evidence suggests that two-tier health care increases public waiting.4
Where private health insurance exists in western Europe, insurance markets are highly regulated and insurers are often non-profit
Across western Europe, private health insurance markets are highly regulated in order to contain costs, maintain affordability, and achieve equity objectives.5 All of the comparator countries have a mandatory public health system or public insurance scheme with public or non-profit insurers that provide universal coverage. None of the countries rely on purely private, for-profit health insurers to provide coverage for medically necessary services, like the Alberta model encourages.
For example, in the Netherlands, a health system that is often held up as an example of “private” involvement, the “strong public role in regulation and finance renders this unique model effective ‘public’.’’6
Another challenge facing jurisdictions with a much greater role for private health insurance is the public cost of regulation and enforcement. France has mandatory public SHI, but has a large market for complementary insurance that helps cover co-payments for health services (there are also supports for lower-income people). Public dollars spent on regulating the private insurance market are dollars that are not spent directly on health care. As scholars of the French system remind us, “this combination of public-private insurance comes with a high management cost: France has the second highest administrative costs (6 per cent of the health spending) in the OECD, just after the United States, and almost half of this expenditure is related to complementary health insurance.”7
OECD countries have a greater share of public financing than Canada
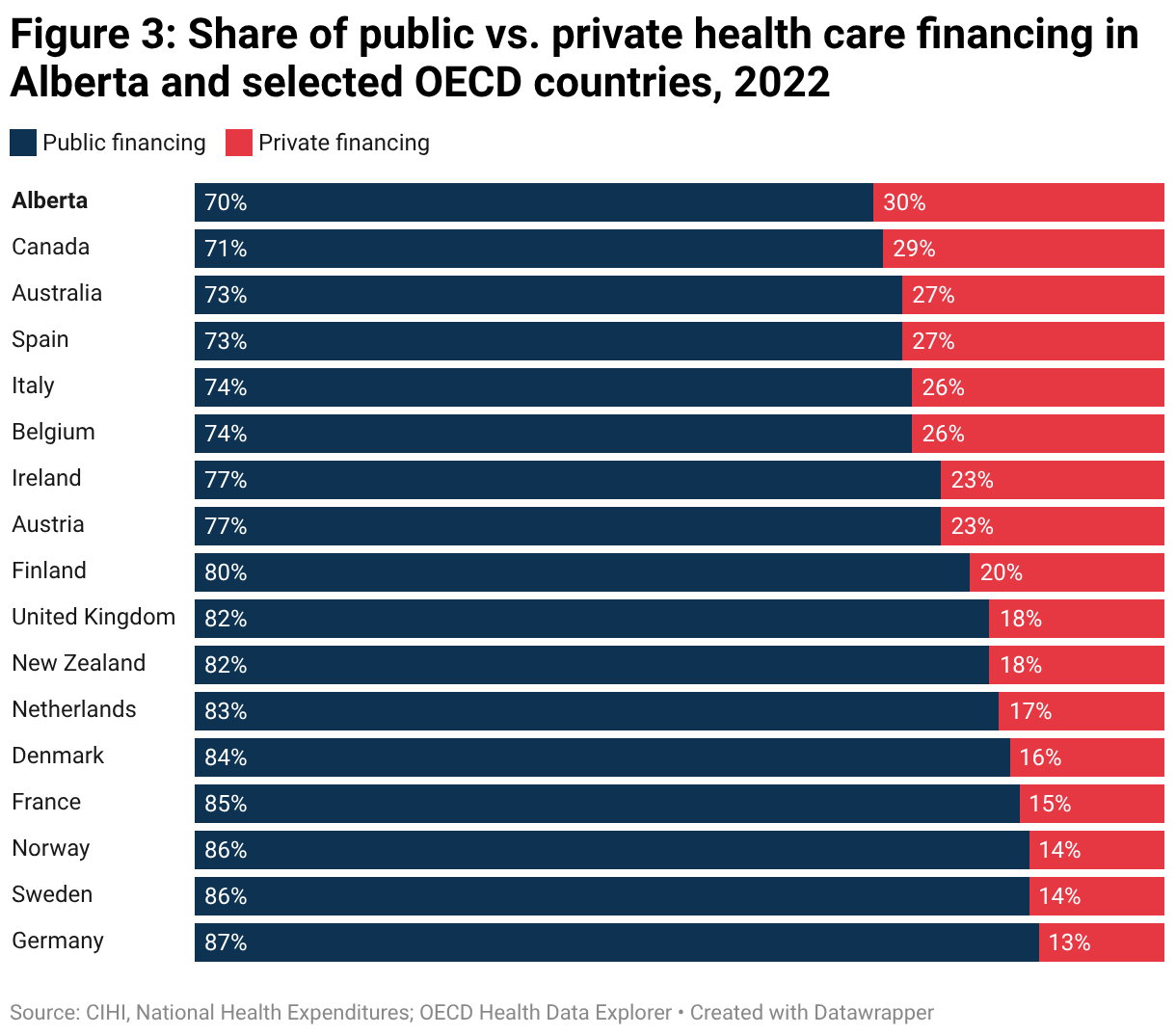
Canada has the largest share of private health care financing among comparable high-income OECD countries. Although the Alberta government suggests that we should be emulating a number of western European countries and Australia for supposed greater private, for-profit involvement, the reality is that public spending represents a greater overall share of health spending in these jurisdictions.
In Canada, 29 per cent of health spending is private (30 per cent in Alberta), which declines to 27 per cent in Australia and Spain, 18 per cent in the UK, 17 per cent in the Netherlands, and 13 per cent in Germany. Rather than market utopias, as the Alberta government seems to suggest, these health systems have more extensive public coverage of health services, prescription drugs, and seniors’ care. It’s not a story about private involvement, but these health systems demonstrate a greater commitment to public financing and coverage.
Making sense of health system comparisons
International health system comparisons are complex. The Alberta government is guilty of “drive-by” comparisons that decontextualize the complex interactions between public and private financing as well as public and private delivery of services. Health systems have evolved over hundreds of years and reflect their unique political culture, legislation, and policy contexts. As this analysis has shown, dual physician practice based on the Alberta approach—allowing physicians to simultaneously work in the public system and private-pay market—does not exist in western European health systems. Rather, these countries exhibit a greater commitment to public financing and regulation than the Canadian provinces.
Instead of moving Alberta closer to European jurisdictions, Bill 11 encourages the growth of a U.S.-style private health insurance market for all health care services that Albertans—and Canadians—rely on. Alberta is the first Canadian province to introduce two-tier legislation and encourage a private health insurance market for services covered under the Canada Health Act. This is a decisive shift towards U.S. health care based on greed and profit-taking, not “European” health care based largely on principles of social solidarity and universality.
Appendix: Characteristics of selected international health systems and Alberta
Alberta
Type of system: Under Bill 11, provincial public health insurance will exist with duplicative private health insurance, contrary to Canada Health Act
Primary health insurance financing: General tax revenue, mainly provincial but also federal transfers. Unlikely to change under Bill 11.
Secondary health insurance and out-of-pocket payment financing:8 Bill 11 will likely encourage a mix of employer-sponsored duplicative private health insurance, out-of-pocket payment for surgeries and diagnostics, and some individual private health insurance.
Australia
Type of system: National public health insurance9
Primary health insurance financing: General tax revenue; earmarked income tax (Medicare levy).10
Secondary health insurance and out-of-pocket payment financing:11 Complementary and duplicative coverage for faster access. 46% have hospital coverage. Private insurance heavily subsidized by government through means-tested tax rebates. HIgh earners face penalty for not having private insurance.
Denmark
Type of system: National health care system12
Primary health insurance financing: Mostly national income taxes; 20% from municipal and state block grants.13
Secondary health insurance and out-of-pocket payment financing:14 42% purchase complementary non-profit coverage; 30% have duplicative for-profit coverage, mainly through employer, for expanded access to private providers.15
France
Type of system: Social insurance model: Statutory insurance provided by non-competitive, employment-based funds. Tax-financed coverage for unemployed.16
Primary health insurance financing: Multiple sources: employer/employee payroll tax, income taxes, general and earmarked taxes.
Secondary health insurance and out-of-pocket payment financing:17 95% have complementary coverage from non-profit insurers, either through employer or means-tested government vouchers. Limited insurance by for-profit insurers.
Germany
Type of system: Social insurance model: Statutory/mandatory insurance provided by 109 non-profit “sickness funds” covering 88% of population. Wealthy may opt for fully private insurance.
Primary health insurance financing: Sickness funds: compulsory wage contributions from employers/employees and distributed to sickness funds.
Secondary health insurance and out-of-pocket payment financing:18 Sickness fund enrollees may purchase duplicative and complementary insurance covering minor benefits not covered by sickness funds. Duplicative insurance is an alternative to the public social health insurance scheme, and once opted in, it is very difficult to return to the public scheme.
Netherlands
Type of system: Social insurance model: Statutory/mandatory insurance offered through 11 non-profit insurers.
Primary health insurance financing: Earmarked payroll tax (employers); community-rated insurance premiums (individuals); general tax revenue; government grants.
Secondary health insurance and out-of-pocket payment financing:19 84% buy supplementary coverage for benefits excluded from statutory package (dental care, physio, eyeglasses).
Spain
Type of system: National health care system (SNS), managed by regions
Primary health insurance financing: Mostly general tax revenue
Secondary health insurance and out-of-pocket payment financing:20 20% buy duplicative or complementary coverage for faster access to hospital and specialist care and for services not covered by the statutory plan.
England
Type of system: National health care system (NHS England)
Primary health insurance financing: Mostly general tax revenue; 20% from national insurance, a payroll tax shared between employers and employees.
Secondary health insurance and out-of-pocket payment financing:21 11% buy duplicative coverage for faster access
![[ Insert title here ] (Table)](https://datawrapper.dwcdn.net/wfnc7/full.png)
link




