
Korea’s Healthcare System Part I: Why Are Doctors Going on Strike?

Korea’s Healthcare System Part I: Why Are Doctors Going on Strike?

Korea stands out for its long life expectancy of 83.6 years as of 2021, the second longest among the 38 countries that are members of the OECD. In addition, its avoidable mortality rate (premature death from preventable and treatable causes) was 142 per 100,000 persons, well below the OECD average. Expanded access to healthcare has helped lengthen longevity and improve health conditions. However, a number of issues, including doctor shortages, suggest the need for reforms.
Concern about Doctor Shortages
The government announced measures in February 2024 to upgrade the healthcare system by spending over KRW 10 trillion (0.4% of GDP) to improve essential services, especially in rural areas, and to boost medical school admissions from 3,000 to 5,000 annually, beginning in 2025. The admissions quota has not been increased in 27 years despite government efforts since 2006 to raise it. The planned increase would mean an additional 10,000 doctors in a decade. Korea’s doctor shortage is primarily in high-risk, low-pay fields, such as pediatrics and obstetrics, and emergency care. In addition, there are regional mismatches between healthcare needs and medical personnel, who are concentrated in the Seoul metropolitan area. Indeed, there are 4.7 doctors per 1,000 people in Seoul. However, nationwide, Korea had only 2.7 practicing doctors per 1,000 population in 2021, the fourth lowest among OECD countries (Figure 1). A previous attempt in 2020 to boost medical school admissions by 400 annually led to a month-long strike doctors strike during the pandemic.
The February plan to raise medical school admissions met strong opposition from doctors, particularly interns and residents (trainee doctors), who complain of harsh working conditions and low wages. They often work over 80 hours a week and make up a third or more of the workforce in some major hospitals. By early March 2024, more than 11,000 trainee doctors were on strike, disrupting healthcare services. In May, the government lowered the planned medical school admissions in 2025 from 5,000 to 4,570. However, by mid-June, only 7.5% the approximately 14,000 interns and residents at 211 teaching hospitals were at work, according to the government. Some senior hospital doctors and professors at medical schools joined the strike in June. To reduce the strains on the healthcare system, the government has deployed military doctors and requested that nurses perform some tasks typically carried out by doctors.
Increasing medical school admissions to reduce doctor shortages would also help prepare for Korea’s rapid population aging, which will significantly boost demand for healthcare. The current number of medical school graduates – 7.3 per 100,000 population, only half the OECD average (Figure 2) – would leave Korea poorly prepared for an aged society. However, increasing the uptake of medical schools may not necessarily resolve the shortages in specific fields, which reflect the structure of the healthcare system. Most care is provided by private providers who are paid on a fee-for-service system by the National Health Insurance (NHI), which provides universal coverage. Raising the fees for fields where the number of doctors is inadequate would help reduce shortages, as new doctors naturally prefer specialties with better pay and working conditions. The current crisis provides an opportunity to discuss fundamental reforms to improve the healthcare system, including changing the payment system.

Reforming the Payment System for Outpatient Care
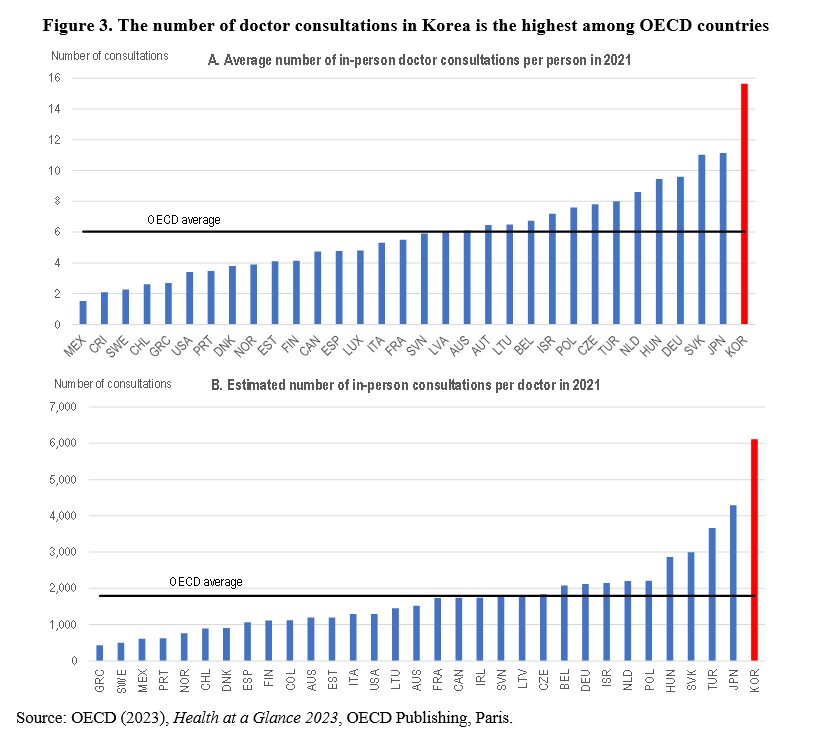
Under the pay-for-fee system, doctors’ income depends on the volume of services they provide at the price set by the NHI. This payment method incentivizes doctors to increase the volume of health services they provide, leading to frequent consultations with patients. Indeed, the average number of in-person doctor consultations per person in Korea rose from 3.7 in 1977 to 15.7 in 2021, 2.6 times the OECD average (Figure 3, Panel A), reflecting revenue-maximizing behaviour by health providers. Other countries that rely primarily on a fee-for-service payment system, such as Germany and Japan, also have a high number of consultations per person. Given Korea’s relatively small number of doctors, the estimated number of in-person consultations per doctor was 6,113 in 2021, 3.4 times the OECD average (Panel B). Frequent doctor visits have negative implications for patients, such as more travel to appointments, longer wait times, shorter consultations and higher out-of-pocket payments. For doctors, it means very long working hours, reducing their job satisfaction and creating stress. In sum, the current approach damages doctor-patient relationships and doctor strikes may aggravate this.
Changing the economic incentives for healthcare providers by reforming the payment system is crucial to reducing the number of supplier-induced consultations. Some countries with low doctor consultation rates, such as Denmark and Norway, use a mixture of fee-for-service with capitation payment systems, which pay doctors based on the number of patients rather than on the number of consultations. In a capitation system, healthcare providers receive a fixed payment per enrolled patient over a specific time period and are responsible for delivering all necessary medical services to their patients. This system incentivizes doctors to focus on preventive care, carefully manage chronic diseases, and to choose cost-effective treatment strategies that control healthcare costs. In other words, it encourages healthcare providers to concentrate on quality and efficiency in providing care rather than the quantity of services rendered. However, capitation may incentivize providers to select healthier patients, as they are less likely to require costly medical services, leading to disparities in access to medical care and health outcomes between different patient populations. Consequently, a capitation system should adjust for risk factors, such as patients’ age and health status, to discourage healthcare providers from “cherry-picking” low-risk patients and providing less healthcare than optimal.
Other Policies to Reduce the High Number of Doctor Consultations
Although the United States relies mainly on a fee-for-service payment system, the number of doctor consultations is relatively low, which may reflect two factors. First, many patients face high out-of-pocket payments due to co-payments, which prompts them to limit the number of consultations with doctors because of the cost. However, out-of-pocket payments are already exceptionally high in Korea at 29% of total health expenditure in 2021, far above the OECD average of 18%. Further increasing out-of-pocket payments would adversely affect lower-income households and persons with chronic diseases. Second, the low number of doctor consultations in the United States is partly due to the key role that nurses and other health professionals play in primary care, such as minor health issues and chronic illnesses. Such an approach may be helpful in Korea, which has 8.8 nurses per 1,000 population, close to the OECD average of 9.2.
Another option is greater use of telemedicine – information and communication technology (ICT) to provide healthcare at a distance, often through video calls with patients. Many countries adopted policies to promote the use of telemedicine during the COVID-19 pandemic, which caused significant disruptions to in-person care. Before March 2020, nine of the 38 OECD countries required medical consultations to be performed in the physical presence of patients. Since then, all OECD countries, except Korea, abolished this requirement. Although Korea made it possible to use telemedicine services on a temporary basis during the pandemic, telemedicine is strictly limited to exceptional situations needed to limit the transmission of infectious diseases in hospitals.
As a world leader in ICT, Korea is well-positioned to benefit from telemedicine. Its ICT sector accounts for significant shares of value added and employment and drives innovation. Korea’s high level of R&D in ICT leads to more ICT-related patents (as a share of total IP5 patent families) than any other OECD country. In addition, Korea outpaces many OECD countries in fixed and mobile broadband networks. Telemedicine would particularly benefit Korea’s elderly population, given that a quarter of them live in rural areas. Telemedicine would thus enhance access to healthcare for those who need it most.
However, telemedicine faces significant resistance from the Korea Medical Association (KMA). Following the introduction of legislation in 2014 to allow it, the KMA threatened to strike. Opposition to telemedicine is based on several arguments. First, telemedicine could lead to misdiagnoses of patients and the theft of personal data. Second, it could hurt smaller medical clinics, which do not have the resources to invest in telemedicine and rely on close geographical proximity to their patients. If telemedicine were permitted, many small clinics would be replaced by doctors in major hospitals in urban areas. The closure of small clinics would ultimately reduce access to essential in-person healthcare. Third, telemedicine could create a market for “smart” technologies available only to those who can afford them. Such issues need to be resolved before telemedicine can be broadly used in Korea.
Conclusion
Increasing the number of doctors is a priority to meet the current shortage and prepare for rapid population aging, increasing the demand for healthcare. The strong opposition of doctors suggests a need for more fundamental reforms, notably by improving the payment system to reduce the number of doctor consultations and enhance the efficiency of healthcare. Enlarging the role of nurses in treating some minor health issues and allowing telemedicine would also mitigate the shortage of doctors.
Randall S. Jones is a Non-Resident Distinguished Fellow at the Korea Economic Institute of America. The views expressed here are the author’s alone.
Photo from Shutterstock.
KEI is registered under the FARA as an agent of the Korea Institute for International Economic Policy, a public corporation established by the government of the Republic of Korea. Additional information is available at the Department of Justice, Washington, D.C.
link





